Shoe Lifts The Solution To Leg Length Discrepancy
There are actually two different types of leg length discrepancies, congenital and acquired. Congenital implies that you are born with it. One leg is anatomically shorter than the other. As a result of developmental phases of aging, the brain picks up on the walking pattern and identifies some variation. The human body typically adapts by dipping one shoulder over to the "short" side. A difference of under a quarter inch is not blatantly irregular, doesn't need Shoe Lifts to compensate and commonly won't have a serious effect over a lifetime.

Leg length inequality goes typically undiscovered on a daily basis, however this issue is very easily remedied, and can eliminate a number of incidents of back ache.
Treatment for leg length inequality commonly consists of Shoe Lifts . Many are very inexpensive, often costing less than twenty dollars, compared to a custom orthotic of $200 or higher. Differences over a quarter inch can take their toll on the spine and should probably be compensated for with a heel lift. In some cases, the shortage can be so extreme that it requires a full lift to both the heel and sole of the shoe.
Chronic back pain is easily the most prevalent health problem afflicting people today. Over 80 million people suffer from back pain at some stage in their life. It's a problem which costs companies millions of dollars annually due to lost time and productivity. New and better treatment methods are always sought after in the hope of lowering economic impact this condition causes.

People from all corners of the world suffer from foot ache due to leg length discrepancy. In a lot of these situations Shoe Lifts can be of worthwhile. The lifts are capable of easing any discomfort and pain in the feet. Shoe Lifts are recommended by countless qualified orthopaedic physicians.
So that they can support the body in a well-balanced manner, feet have got a critical job to play. Inspite of that, it is often the most overlooked zone in the body. Many people have flat-feet meaning there may be unequal force placed on the feet. This will cause other areas of the body like knees, ankles and backs to be impacted too. Shoe Lifts ensure that appropriate posture and balance are restored.
Leg length inequality goes typically undiscovered on a daily basis, however this issue is very easily remedied, and can eliminate a number of incidents of back ache.
Treatment for leg length inequality commonly consists of Shoe Lifts . Many are very inexpensive, often costing less than twenty dollars, compared to a custom orthotic of $200 or higher. Differences over a quarter inch can take their toll on the spine and should probably be compensated for with a heel lift. In some cases, the shortage can be so extreme that it requires a full lift to both the heel and sole of the shoe.
Chronic back pain is easily the most prevalent health problem afflicting people today. Over 80 million people suffer from back pain at some stage in their life. It's a problem which costs companies millions of dollars annually due to lost time and productivity. New and better treatment methods are always sought after in the hope of lowering economic impact this condition causes.
People from all corners of the world suffer from foot ache due to leg length discrepancy. In a lot of these situations Shoe Lifts can be of worthwhile. The lifts are capable of easing any discomfort and pain in the feet. Shoe Lifts are recommended by countless qualified orthopaedic physicians.
So that they can support the body in a well-balanced manner, feet have got a critical job to play. Inspite of that, it is often the most overlooked zone in the body. Many people have flat-feet meaning there may be unequal force placed on the feet. This will cause other areas of the body like knees, ankles and backs to be impacted too. Shoe Lifts ensure that appropriate posture and balance are restored.
What May Cause Posterior Calcaneal Spur

Overview
Heel spur is a hook of bone that forms on the heel bone. The condition itself is not the most painful; it is the inflammation and irritation that cause the heel pain. Often times, plantar fasciitis is a cause of heel spurs. When the ligaments are pulled away, calcium deposits form on the hooked bone. An orthotic will help relieve the pain associated with heel spurs.
Causes
A major cause of heel spur pain comes from the development of new fibrous tissue around the bony spur, which acts as a cushion over the area of stress. As this tissue grows, a callus forms and takes up even more space than the heel spur, leading to less space for the thick surrounding network of tendons, nerves, ligaments and supporting tissue. These important structures in the foot have limited space because of calcium or tissue buildup, which leads to swelling and redness of the foot, and a deep throbbing pain worsened with exercise.
Symptoms
Heel spur and plantar fasciitis pain usually begins in the bottom of the heel, and frequently radiates into the arch. At times, however, the pain may be felt only in the arch. The pain is most intense when first standing, after any period of rest. Most people with this problem experience their greatest pain in the morning, with the first few steps after sleeping. After several minutes of walking, the pain usually becomes less intense and may disappear completely, only to return later with prolonged walking or standing. If a nerve is irritated due to the swollen plantar fascia, this pain may radiate into the ankle. In the early stages of Heel Spurs and Plantar Fasciitis, the pain will usually subside quickly with getting off of the foot and resting. As the disease progresses, it may take longer periods of time for the pain to subside.
Diagnosis
A heel spur is often seen on X-ray as a bony protrusion, which can vary in size. However, because a Heel Spur only indicates increased load on the plantar fascia, and not pain, an ultra sound may be required to assess other actual cause of the heel pain such and may include checking to see if the plantar fascia is inflamed or degenerated.
Non Surgical Treatment
Since heel spurs are not an indication of pain themselves unless fractured, treatment is usually aimed at the cause of the pain which in many cases is plantar fasciosis. Treatment of plantar fasciiosis includes; rest until the pain subsides, special stretching exercises and if required orthotics may be prescribed.
Surgical Treatment
Have surgery if no other treatments work. Before performing surgery, doctors usually give home treatments and improved footwear about a year to work. When nothing else eases the pain, here's what you need to know about surgical options. Instep plantar fasciotomy. Doctors remove part of the plantar fascia to ease pressure on the nerves in your foot. Endoscopy. This surgery performs the same function as an instep plantar fasciotomy but uses smaller incisions so that you'll heal faster. However, endoscopy has a higher rate of nerve damage, so consider this before you opt for this option. Be prepared to wear a below-the-knee walking cast to ease the pain of surgery and to speed the healing process. These casts, or "boots," usually work better than crutches to speed up your recovery time.
Prevention
In order to prevent heel spurs, it?s important that you pay attention to the physical activities you engage in. Running or jogging on hard surfaces, such as cement or blacktop, is typical for competitive runners, but doing this for too long without breaks can lead to heel spurs and foot pain. Likewise, the shoes you wear can make a big difference in whether or not you develop heel spurs. Have your shoes and feet checked regularly by our Dallas podiatrist to ensure that you are wearing the proper equipment for the activities. Regular checkups with a foot and ankle specialist can help avoid the development of heel spurs.
Exactly What Is Inferior Calcaneal Spur

Overview
Patients and doctors often confuse the terms heel spur and plantar fasciitis. While these two diagnoses are related, they are not the same. Plantar fasciitis refers to the inflammation of the plantar fascia--the tissue that forms the arch of the foot. A heel spur is a hook of bone that can form on the heel bone (calcaneus) and is associated with plantar fasciitis. About 70 percent of patients with plantar fasciitis have a heel spur that can be seen on an X-ray. However, many patients without symptoms of pain can have a heel spur. The exact relationship between plantar fasciitis and heel spurs is not entirely understood.
Causes
The cause of heel spurs is excessive strain placed on the plantar fascia over a long period of time, as a result of different factors. These factors include incorrect gait, being overweight, ageing or being in a job that requires a lot of standing on hard floors. It is usually a combination of any of these factors that will bring on the development of heel spurs.

Symptoms
The vast majority of people who have heel spurs feel the asscociated pain during their first steps in the morning. The pain is quite intense and felt either the bottom or front of the heel bone. Typically, the sharp pain diminishes after being up for a while but continues as a dull ache. The pain characteristically returns when first standing up after sitting for long periods.
Diagnosis
A Heel Spur diagnosis is made when an X-ray shows a hook of bone protruding from the bottom of the foot at the point where the plantar fascia is attached to the heel bone. The plantar fascia is the thick, connective tissue that runs from the calcaneus (heel bone) to the ball of the foot. This strong and tight tissue helps maintain the arch of the foot. It is also one of the major transmitters of weight across the foot as you walk or run. In other words, tremendous stress is placed on the plantar fascia.
Non Surgical Treatment
In case of heel spurs rest is most important. Active sports, running, long walks etc should be avoided to start with. If you?re in a job that requires a lot of standing, take a few days off work. Rest (or reduced activity) is essential to allow the inflammation from becoming aggrevated. Furthermore, you can use ice packs (placed on the heel for 5-10 minutes) to ?cool down? the inflamed area. You may take anti-inflammatory medication or apply a topical inflammatory (i.e. a cream) to help reduce inflammation. In addition, there are some simple exercises that should be done daily to help relieve heel spur pain.
Surgical Treatment
Heel spur surgery should only be considered after less invasive treatment methods have been explored and ruled insufficient. The traditional surgical approach to treating heel spurs requires a scalpel cut to the bottom of the food which allows the surgeon to access the bone spur. Endoscopic plantar fasciotomies (EPF) involve one or two small incisions in the foot which allow the surgeon to access and operate on the bone spur endoscopically. Taking a surgical approach to heel spur treatment is a topic to explore with a foot and ankle specialist.
Bursitis Of The Feet Pain In Heel
Overview
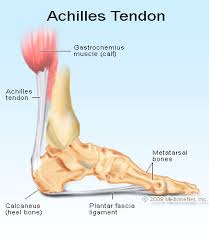
Retrocalcaneal bursitis is a condition characterized by tissue damage and inflammation of the retrocalcaneal bursa (a small fluid filled sac located at the back of the heel) causing pain in the heel region. A bursa is a thin fluid filled sac found in various places throughout the body. Bursae are designed to reduce friction between adjacent layers of tissue and are filled with lubricating fluid. They are typically located in regions of the body where tissue layers may rub against each other or against bony prominences The muscle group at the back of the lower leg is commonly called the calf. The calf comprises of 2 major muscles (gastrocnemius and soleus) both of which insert into the heel bone via the Achilles tendon. Between the Achilles tendon and the heel bone lies a bursa known as the retrocalcaneal bursa.
Causes
Repetitive, vigorous movement, strenuous and unaccustomed activities that put pressure on a joint, or a blow or other injury can bring on bursitis. The cause can vary depending on where the bursitis occurs. In the shoulder, for example, it can be brought on by excessive strain, such as from serving in tennis. Kneeling on a hard floor can cause bursitis of the knee, and similarly, repeatedly resting the elbow on a hard surface (such as a desk) can cause bursitis in that joint. Arthritis, gout, and certain infections can also contribute to the problem. Bursitis, in fact, may signal the onset of arthritis. While getting older isn't a cause of bursitis, older people, especially older athletes, are more likely to develop the condition.
Symptoms
Patients with this condition typically experience pain at the back of the ankle and heel where the Achilles tendon attaches into the heel bone. Pain is typically experienced during activities requiring strong or repetitive calf contractions (often involving end of range ankle movements) such as walking (especially uphill), going up and down stairs, running, jumping or hopping (especially whilst wearing excessively tight shoes). Often pain may be worse with rest after these activities (especially that night or the following morning). The pain associated with this condition may 'warm up' with activity in the initial stages of injury. As the condition progresses, patients may experience symptoms that increase during sport or activity, affecting performance. In severe cases, patients may walk with a limp or be unable to weight bear on the affected leg. Other symptoms may include tenderness on firmly touching the affected bursa and swelling around the Achilles region.
Diagnosis
When a patient has pain in a joint, a careful physical examination is needed to determine what type of movement is affected and if there is any swelling present. Bursitis will not show up on x-rays, although sometimes there are also calcium deposits in the joint that can be seen. Inserting a thin needle into the affected bursa and removing (aspirating) some of the synovial fluid for examination can confirm the diagnosis. In most cases, the fluid will not be clear. It can be tested for the presence of microorganisms, which would indicate an infection, and crystals, which could indicate gout. In instances where the diagnosis is difficult, a local anesthetic (a drug that numbs the area) is injected into the painful spot. If the discomfort stops temporarily, then bursitis is probably the correct diagnosis.
Non Surgical Treatment
The most important part of treating bursitis is resting your Achilles tendon while the bursa heals. Resting your ankle as much as possible may decrease swelling and keep the bursitis from getting worse. When the pain decreases, begin normal, slow movements. Ice causes blood vessels to constrict (get small) which helps decrease inflammation (swelling, pain, and redness). Put crushed ice in a plastic bag or use a bag of frozen corn or peas. Cover it with a towel. Put this on your heel for 15 to 20 minutes, three to four times each day. Do not sleep on the ice pack because you can get frostbite. After two or three days, you may try using heat to decrease pain and stiffness. Use a hot water bottle, heating pad, whirlpool or warm, moist compress. To make a compress, dip a clean washcloth in warm water. Wring out the extra water and put it on your heel for 15 to 20 minutes, three to four times each day. Your caregiver may tell you to switch between treating your heel with ice packs and heat treatments. Follow the caregiver's directions carefully when doing these treatments.
Surgical Treatment
Surgery is rarely need to treat most of these conditions. A patient with a soft tissue rheumatic syndrome may need surgery, however, if problems persist and other treatment methods do not help symptoms.
Prevention
People can lower the risk of bursitis by gradually strengthening and stretching the muscles around the joints and taking regular breaks from repetitive motion that might irritate bursae. Prolonged time resting on the elbows or kneeling should be avoided, if it cannot be avoided, wearing cushioned elbow and knee pads can help protect the bursae. Comfortable, supportive, low-heeled shoes can help prevent bursitis in the foot.
Retrocalcaneal bursitis is a condition characterized by tissue damage and inflammation of the retrocalcaneal bursa (a small fluid filled sac located at the back of the heel) causing pain in the heel region. A bursa is a thin fluid filled sac found in various places throughout the body. Bursae are designed to reduce friction between adjacent layers of tissue and are filled with lubricating fluid. They are typically located in regions of the body where tissue layers may rub against each other or against bony prominences The muscle group at the back of the lower leg is commonly called the calf. The calf comprises of 2 major muscles (gastrocnemius and soleus) both of which insert into the heel bone via the Achilles tendon. Between the Achilles tendon and the heel bone lies a bursa known as the retrocalcaneal bursa.
Causes
Repetitive, vigorous movement, strenuous and unaccustomed activities that put pressure on a joint, or a blow or other injury can bring on bursitis. The cause can vary depending on where the bursitis occurs. In the shoulder, for example, it can be brought on by excessive strain, such as from serving in tennis. Kneeling on a hard floor can cause bursitis of the knee, and similarly, repeatedly resting the elbow on a hard surface (such as a desk) can cause bursitis in that joint. Arthritis, gout, and certain infections can also contribute to the problem. Bursitis, in fact, may signal the onset of arthritis. While getting older isn't a cause of bursitis, older people, especially older athletes, are more likely to develop the condition.
Symptoms
Patients with this condition typically experience pain at the back of the ankle and heel where the Achilles tendon attaches into the heel bone. Pain is typically experienced during activities requiring strong or repetitive calf contractions (often involving end of range ankle movements) such as walking (especially uphill), going up and down stairs, running, jumping or hopping (especially whilst wearing excessively tight shoes). Often pain may be worse with rest after these activities (especially that night or the following morning). The pain associated with this condition may 'warm up' with activity in the initial stages of injury. As the condition progresses, patients may experience symptoms that increase during sport or activity, affecting performance. In severe cases, patients may walk with a limp or be unable to weight bear on the affected leg. Other symptoms may include tenderness on firmly touching the affected bursa and swelling around the Achilles region.
Diagnosis
When a patient has pain in a joint, a careful physical examination is needed to determine what type of movement is affected and if there is any swelling present. Bursitis will not show up on x-rays, although sometimes there are also calcium deposits in the joint that can be seen. Inserting a thin needle into the affected bursa and removing (aspirating) some of the synovial fluid for examination can confirm the diagnosis. In most cases, the fluid will not be clear. It can be tested for the presence of microorganisms, which would indicate an infection, and crystals, which could indicate gout. In instances where the diagnosis is difficult, a local anesthetic (a drug that numbs the area) is injected into the painful spot. If the discomfort stops temporarily, then bursitis is probably the correct diagnosis.
Non Surgical Treatment
The most important part of treating bursitis is resting your Achilles tendon while the bursa heals. Resting your ankle as much as possible may decrease swelling and keep the bursitis from getting worse. When the pain decreases, begin normal, slow movements. Ice causes blood vessels to constrict (get small) which helps decrease inflammation (swelling, pain, and redness). Put crushed ice in a plastic bag or use a bag of frozen corn or peas. Cover it with a towel. Put this on your heel for 15 to 20 minutes, three to four times each day. Do not sleep on the ice pack because you can get frostbite. After two or three days, you may try using heat to decrease pain and stiffness. Use a hot water bottle, heating pad, whirlpool or warm, moist compress. To make a compress, dip a clean washcloth in warm water. Wring out the extra water and put it on your heel for 15 to 20 minutes, three to four times each day. Your caregiver may tell you to switch between treating your heel with ice packs and heat treatments. Follow the caregiver's directions carefully when doing these treatments.
Surgical Treatment
Surgery is rarely need to treat most of these conditions. A patient with a soft tissue rheumatic syndrome may need surgery, however, if problems persist and other treatment methods do not help symptoms.
Prevention
People can lower the risk of bursitis by gradually strengthening and stretching the muscles around the joints and taking regular breaks from repetitive motion that might irritate bursae. Prolonged time resting on the elbows or kneeling should be avoided, if it cannot be avoided, wearing cushioned elbow and knee pads can help protect the bursae. Comfortable, supportive, low-heeled shoes can help prevent bursitis in the foot.
Hammertoe Correction Surgery
 Overview
Overview
Hammer toe deformities can be painful and unsightly. These toe deformities can be the result of a muscle/tendon imbalance or often the end stage result of some systemic disease such as diabetes or arthritis, especially Rheumatoid arthritis. Hammertoe deformities are progressive and can be prevented.
Causes
Certain risk factors increase your likelihood of developing a hammertoe. These include a family history of hammertoes, wearing tight or pointy-toed shoes, wearing shoes that are too small, having calluses, bunions, or corns (thickened layers of skin caused by prolonged/repeated friction) Wearing shoes that are too small can force the joint of your toes into a dislocated position. This makes it impossible for your muscles to stretch out. Over time, the practice of wearing improperly fitting shoes increases your risk of developing hammertoes, blisters, bunions, and corns.
 Symptoms
Symptoms
Common reasons patients seek treatment for toe problems are toe pain on the knuckle. Thick toe calluses. Interference with walking/activities. Difficulty fitting shoes. Worsening toe deformity. Pain at the ball of the foot. Unsightly appearance. Toe deformities (contractures) come in varying degrees of severity, from slight to severe. The can be present in conjunction with a bunion, and develop onto a severe disfiguring foot deformity. Advanced cases, the toe can dislocate on top of the foot. Depending on your overall health, symptoms and severity of the hammer toe, the condition may be treated conservatively and/or with surgery.
Diagnosis
Most health care professionals can diagnose hammertoe simply by examining your toes and feet. X-rays of the feet are not needed to diagnose hammertoe, but they may be useful to look for signs of some types of arthritis (such as rheumatoid arthritis) or other disorders that can cause hammertoe.
Non Surgical Treatment
Apply a Hammer toes commercial, non-medicated hammer toe pad around the bony prominence of the hammer toe to decrease pressure on the area. Wear a shoe with a deep toe box. If the hammer toe becomes inflamed and painful, apply ice packs several times a day to reduce swelling. Avoid heels more than two inches tall. A loose-fitting pair of shoes can also help protect the foot while reducing pressure on the affected toe, making walking a little easier until a visit to your podiatrist can be arranged. While this treatment will make the hammer toe feel better, it is important to remember that it does not cure the condition. A trip to the podiatrist's office will be necessary to repair the toe to allow for normal foot function. Avoid wearing shoes that are too tight or narrow. Children should have their shoes properly fitted on a regular basis, as their feet can often outgrow their shoes rapidly.
Surgical Treatment
For severe hammer toe, you will need an operation to straighten the joint. The surgery often involves cutting or moving tendons and ligaments. Sometimes the bones on each side of the joint need to be connected (fused) together. Most of the time, you will go home on the same day as the surgery. The toe may still be stiff afterward, and it may be shorter. If the condition is treated early, you can often avoid surgery. Treatment will reduce pain and walking difficulty.
 Prevention
Prevention
The best treatment is good prevention! Hammertoe can be prevented by wearing shoes with ample toe room, avoiding high heels, and wearing adjustable shoes to assure a looser fit. When buying shoes, shop at the end of the day when your feet are swollen from daily activity, try both shoes on to confirm they fit properly, and if necessary, visit a shoe repair store to see if they can stretch your shoes for a better fit.
What Are Hallux Valgus?
Overview
 A bunion is a ?bump? on the joint at the base of the big toe-the metatarsophalangeal (MTP) joint-that forms when the bone or tissue at the big toe joint moves out of place. The toe is forced to bend toward the others, causing an often painful lump of bone on the foot. Because this joint carries a lot of the body's weight while walking, bunions can cause extreme pain if left untreated. The MTP joint itself may become stiff and sore, making even the wearing of shoes difficult or impossible. A bunion-from the Latin "bunio," meaning enlargement, can also occur on the outside of the foot along the little toe, where it is called a "bunionette" or "tailor's bunion".
A bunion is a ?bump? on the joint at the base of the big toe-the metatarsophalangeal (MTP) joint-that forms when the bone or tissue at the big toe joint moves out of place. The toe is forced to bend toward the others, causing an often painful lump of bone on the foot. Because this joint carries a lot of the body's weight while walking, bunions can cause extreme pain if left untreated. The MTP joint itself may become stiff and sore, making even the wearing of shoes difficult or impossible. A bunion-from the Latin "bunio," meaning enlargement, can also occur on the outside of the foot along the little toe, where it is called a "bunionette" or "tailor's bunion".
Causes
Bunions are more common in women than men. The problem can run in families. People born with abnormal bones in their feet are more likely to form a bunion. Wearing narrow-toed, high-heeled shoes may lead to the development of a bunion. The condition may become painful as the bump gets worse. Extra bone and a fluid-filled sac grow at the base of the big toe.
Symptoms
The dominant symptom of a bunion is a big bulging bump on the inside of the base of the big toe. Other symptoms include swelling, soreness and redness around the big toe joint, a tough callus at the bottom of the big toe and persistent or intermittent pain.
Diagnosis
When an x-ray of a bunion is taken, there is usually angulation between the first metatarsal bone and the bones of the big toe. There may also be angulation between the first and second metatarsal bones. These angular irregularities are the essence of most bunions. In general, surgery for bunions aims to correct such angular deformities.
Non Surgical Treatment
If overpronation is diagnosed early enough, the mechanics of the feet can be adjusted using a prescription orthotic. If orthotics are worn consistently, many major foot deformities can be avoided such as bunions. Early detection is of paramount importance. When a bunion progresses and cannot be controlled by an orthotic, surgical correction may be a consideration. Many advances in bunion correction allow for surgical intervention to make healing and return to normal activities much easier than use of traditional bunion surgery. 
Surgical Treatment
Bunion surgery is usually done as an out patient procedure, so the patient does not have to stay in hospital overnight although it is usually performed under a general anesthetic. The procedure involves the surgeon making a cut on the inside of the big toe joint and removing excess bone whilst also repositioning ligaments and tendons. The joint may be fixed with screws or wires, which may be dissolve, or may be removed at a later date or in some cases, remain in the foot permanently. After the operation the foot will be immobilized, often in a cast for 4 to 8 weeks to keep the bones in alignment. Crutches will usually be issued to help the patient get around. After this period, the foot will be assessed to check the bones have healed correctly. At which point full weight bearing may be gradually introduced.
Prevention
If the diagnosis is made early on, such as in preadolescence, bunion development can be slowed and in some cases arrested with the proper supportive shoe gear and custom functional shoe inserts (orthotics). Avoidance of certain athletic activities with improper shoe fit and toe pressure can prevent the symptoms that occur with bunions.
Is Over-Pronation
Overview
Pronation is the inward movement of the foot as it rolls to distribute the force of impact of the ground as you run. The foot "rolls" inward about fifteen percent, comes in complete contact with the ground, and can support your body weight without any problem. Pronation is critical to proper shock absorption, and it helps you push off evenly from the front of the foot. Although pronation is a natural movement of the foot, the size of the arch can affect its ability to roll, causing either supination (underpronation) or overpronation. If you have a normal arch, you're likely a normal pronator, meaning you'll do best in a shoe that offers moderate pronation control. People with flat feet normally overpronate, so they do well in a motion-control shoe that controls pronation. High-arched people typically underpronate, so they do best in a neutral-cushioned shoe that encourages a more natural foot motion.
Causes
It is important to identify the cause of overpronation in order to determine the best treatment methods to adopt. Not all treatments and preventative measures will work equally well for everyone, and there may be a little trial and error involved to get the best treatment. A trip to a podiatrist or a sports therapist will help you to establish the cause of overpronation, and they will be able to tell you the best treatments based on your specific degree of overpronation and the cause. Overpronation has many causes, with the most common reasons for excessive pronation listed, low arches, flexible flat feet, fallen arches, gait abnormalities, abnormal bone structure, abnormal musculature, bunions, corns and calluses.
Symptoms
Over-Pronation may cause pain in the heel of the foot, the foot arch, under the ball of the foot, in the ankle, knee, hip or back. The symptoms may be localized to one particular area of the foot or may be experienced in any number of combinations. Standing for long periods of time, walking and running may become difficult due to the additional stress and/or discomfort accompanied with these activities. Upon Visual Inspection, when standing the heels of the foot lean inward and one or both of the knee caps may turn inward.
Diagnosis
Firstly, look at your feet in standing, have you got a clear arch on the inside of the foot? If there is not an arch and the innermost part of the sole touches the floor, then your feet are over-pronated. Secondly, look at your running shoes. If they are worn on the inside of the sole in particular, then pronation may be a problem for you. Thirdly, try the wet foot test. Wet your feet and walk along a section of paving and look at the footprints you leave. A normal foot will leave a print of the heel, connected to the forefoot by a strip approximately half the width of the foot on the outside of the sole. If you?re feet are pronated there may be little distinction between the rear and forefoot, shown opposite. The best way to determine if you over pronate is to visit a podiatrist or similar who can do a full gait analysis on a treadmill or using forceplates measuring exactly the forces and angles of the foot whilst running. It is not only the amount of over pronation which is important but the timing of it during the gait cycle as well that needs to be assessed.
Non Surgical Treatment
Orthotics are medical devices used to provide support to correct a physical abnormality. They can provide arch support when needed to remedy over-pronation, and in this particular cases the orthoses used are usually convenient shoe inserts. These can be taken in and out of shoes, and will be carefully tailored by your podiatrist to the specifics of your foot. It can take some weeks before the effects of the inserts can become truly noticeable, and in many cases your podiatrist will want to review your orthotics within a few weeks to make fine adjustments based on how well they have worked to reduce your pain.
Surgical Treatment
Subtalar Arthroereisis. The ankle and hindfoot bones/midfoot bones around the joint are fused, locking the bones in place and preventing all joint motion. This may also be done in combination with fusion at other joints. This is a very aggressive option usually reserved for extreme cases where no joint flexibility is present and/or the patient has severe arthritic changes in the joint.
Pronation is the inward movement of the foot as it rolls to distribute the force of impact of the ground as you run. The foot "rolls" inward about fifteen percent, comes in complete contact with the ground, and can support your body weight without any problem. Pronation is critical to proper shock absorption, and it helps you push off evenly from the front of the foot. Although pronation is a natural movement of the foot, the size of the arch can affect its ability to roll, causing either supination (underpronation) or overpronation. If you have a normal arch, you're likely a normal pronator, meaning you'll do best in a shoe that offers moderate pronation control. People with flat feet normally overpronate, so they do well in a motion-control shoe that controls pronation. High-arched people typically underpronate, so they do best in a neutral-cushioned shoe that encourages a more natural foot motion.
Causes
It is important to identify the cause of overpronation in order to determine the best treatment methods to adopt. Not all treatments and preventative measures will work equally well for everyone, and there may be a little trial and error involved to get the best treatment. A trip to a podiatrist or a sports therapist will help you to establish the cause of overpronation, and they will be able to tell you the best treatments based on your specific degree of overpronation and the cause. Overpronation has many causes, with the most common reasons for excessive pronation listed, low arches, flexible flat feet, fallen arches, gait abnormalities, abnormal bone structure, abnormal musculature, bunions, corns and calluses.
Symptoms
Over-Pronation may cause pain in the heel of the foot, the foot arch, under the ball of the foot, in the ankle, knee, hip or back. The symptoms may be localized to one particular area of the foot or may be experienced in any number of combinations. Standing for long periods of time, walking and running may become difficult due to the additional stress and/or discomfort accompanied with these activities. Upon Visual Inspection, when standing the heels of the foot lean inward and one or both of the knee caps may turn inward.
Diagnosis
Firstly, look at your feet in standing, have you got a clear arch on the inside of the foot? If there is not an arch and the innermost part of the sole touches the floor, then your feet are over-pronated. Secondly, look at your running shoes. If they are worn on the inside of the sole in particular, then pronation may be a problem for you. Thirdly, try the wet foot test. Wet your feet and walk along a section of paving and look at the footprints you leave. A normal foot will leave a print of the heel, connected to the forefoot by a strip approximately half the width of the foot on the outside of the sole. If you?re feet are pronated there may be little distinction between the rear and forefoot, shown opposite. The best way to determine if you over pronate is to visit a podiatrist or similar who can do a full gait analysis on a treadmill or using forceplates measuring exactly the forces and angles of the foot whilst running. It is not only the amount of over pronation which is important but the timing of it during the gait cycle as well that needs to be assessed.
Non Surgical Treatment
Orthotics are medical devices used to provide support to correct a physical abnormality. They can provide arch support when needed to remedy over-pronation, and in this particular cases the orthoses used are usually convenient shoe inserts. These can be taken in and out of shoes, and will be carefully tailored by your podiatrist to the specifics of your foot. It can take some weeks before the effects of the inserts can become truly noticeable, and in many cases your podiatrist will want to review your orthotics within a few weeks to make fine adjustments based on how well they have worked to reduce your pain.
Surgical Treatment
Subtalar Arthroereisis. The ankle and hindfoot bones/midfoot bones around the joint are fused, locking the bones in place and preventing all joint motion. This may also be done in combination with fusion at other joints. This is a very aggressive option usually reserved for extreme cases where no joint flexibility is present and/or the patient has severe arthritic changes in the joint.